
Properly timing your child’s phase 2 of orthodontic treatment is an important responsibility of both the orthodontist and the parent. But, there are very few (reliable) resources on the topic available to most parents. Nonetheless, an improperly timed case versus a properly timed case can be the difference between an average result and an excellent result, a case requiring extraction of permanent teeth versus non-extraction, and in rare cases, the difference between requiring jaw surgery or not. My hope is that with these Newsletters, you will be equipped to make well-informed decisions about your child’s phase 2 orthodontic treatment. You may even be able to help out a friend, too!
Last time, I talked about timing treatment with loss of the last few baby teeth, and the space that can be gained by controlling that process. This time, I am talking about the adolescent growth spurt, and how it affects treatment.
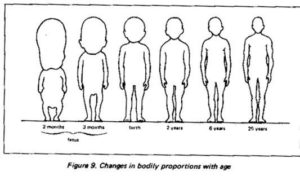 First off, let’s talk about this thing called the cephalocaudal growth gradient. The prefix “ceph” comes from a Greek word for “head,” and the prefix “caud” comes from a Greek word for “tail.” So basically, head-to-tail growth gradient. If you picture a newborn baby, with their cute little feet and big heads, you can’t help but smile. But you will notice, their head is like a third of the entire body! And then compare that to an adult, whose body is much larger proportionally than the head. The principle is that as you move down the body, away from the head and towards the “tail,” growth occurs for a longer time and in greater magnitude for the “tail-end” structures.
First off, let’s talk about this thing called the cephalocaudal growth gradient. The prefix “ceph” comes from a Greek word for “head,” and the prefix “caud” comes from a Greek word for “tail.” So basically, head-to-tail growth gradient. If you picture a newborn baby, with their cute little feet and big heads, you can’t help but smile. But you will notice, their head is like a third of the entire body! And then compare that to an adult, whose body is much larger proportionally than the head. The principle is that as you move down the body, away from the head and towards the “tail,” growth occurs for a longer time and in greater magnitude for the “tail-end” structures.

The cool thing is, this phenomenon occurs on more local levels as well. Back to the cute baby face, you may also notice that they have hardly any chin. The lower jaw is underdeveloped at birth, but throughout childhood and adolescence, it will outgrow the upper jaw. This is called differential jaw growth, but it’s really a localized example of the cephalocaudal growth gradient.
This growth gradient occurs from infancy until adulthood, with growth spurts and growth pauses along the way. The adolescent growth spurt is kind of the big one for orthodontists. It is the last one to occur before adulthood, and during this period of time your child will undergo dramatic changes. The relative growth rate of their lower jaw will skyrocket, and that growth is the single most effective tool for correcting many malocclusions.
Orthodontists are limited in how far we can move teeth by the position of the jaws. The teeth need to stay within the jaws. But, if we can time treatment in a way that incorporates the adolescent growth spurt, your orthodontist can see where the teeth are currently, where they might be as a result of growth, and make the appropriate interventions. Our range of tooth-movement possibilities is dramatically increased because we have essentially gotten nature on our side to do the heavy lifting.
You may even have heard of an orthodontic appliance called a “Herbst,” or a “MARA,” and there are a handful of others which operate on the same principle. The idea is that they supposedly stimulate even more jaw growth during the growth spurt. Whether or not they actually work that way is debatable and orthodontists argue about it all the time. I will probably write about in the future, and get half of my colleagues riled up.
Like the loss of baby teeth, though, the adolescent growth spurt occurs at different ages for different kids. So how do we plan for it in our treatment? There are “average” ages that growth spurts occur, but averages are not very useful when planning for an individual. Especially when the bell curve is pretty wide. In the next article, I will describe the science and techniques that we use to predict growth patterns. I have found that parents are often intrigued when I tell them how I know when their child is about to hit a growth spurt, and I think that it will be an interesting read for all of you!